

A multidisciplinary team, including Dr. James D. Slover and Dr. Ran Schwarzkopf, explores the most effective strategies for treating orthopedic diseases.
Photo: NYU Langone Staff
To raise the quality of orthopedic care for all patients, doctors at NYU Langone Orthopedic Hospital conduct patient safety and outcomes research, with a particular interest in understanding the factors that drive healthcare value. Here are some highlights of recent efforts designed to identify the most effective strategies for treating orthopedic diseases, optimizing patient safety and outcomes, and controlling total costs.
Does Same-Day Discharge for ACDF Increase Unplanned Admissions?
A growing number of anterior cervical discectomy and fusion (ACDF) surgeries are being performed in the outpatient setting. Various studies have demonstrated that outpatient ACDF surgery is both safe and effective and has comparable complication, reoperation, unplanned admission, and mortality rates to inpatient ACDF. In addition, outpatient ACDF is typically more cost-effective. It is estimated that widespread adoption of this approach could lead to annual national savings of up to $140 million. For all these reasons, it is likely that insurance companies will create incentives that convert the majority of ACDFs to outpatient procedures in the near future. As a result, it is paramount that hospitals develop protocols to ensure that same-day ACDF is carried out safely.
At NYU Langone, a multidisciplinary task force developed a protocol for same-day discharge (SDD) ACDF. The protocol utilizes strict inclusion criteria, multiple assessments, and structured observation to ensure safe discharge of ACDF patients on postoperative day 0. The team hypothesized that using the protocol to identify ACDF patients for SDD would result in a non-inferior unplanned admission rate compared to traditional same-day admission (SDA).
According to the new protocol, SDD is only open to patients indicated for primary one- or two-level ACDF. In addition, the patient must be younger than 65; have a body mass index (BMI) less than 35 and an American Society of Anesthesiologists’ (ASA) score of less than 3; and have no history of cerebrovascular accident (CVA), transient ischemic attack (TIA), coagulopathy, or bleeding diathesis. The patient’s operative time must have been less than 180 minutes without complications. Eligible patients are monitored in the post-anesthesia care unit (PACU) for a minimum of four hours and must be without any complications or concerns from the anesthesia, nursing, and surgical teams before discharge.
To evaluate the protocol, the team performed a retrospective chart review of 434 patients who underwent one- or two-level ACDF from March 2016 to March 2017. The review excluded patients who underwent cervical disc replacement, a hybrid procedure, surgery at three or more levels, corpectomy, or a posterior or revision procedure. Data extracted included age, gender, BMI, date of surgery, discharge date, surgical procedure, surgical time, and recovery room time.
Of the patients reviewed, 126 were discharged on the day of surgery and categorized as SDD while 308 patients were admitted to the hospital immediately after surgery and categorized as SDA. Once admitted, 77 percent were discharged on postoperative day 1, with the average length of stay being 1.48 days.
Overall, only three patients experienced an unplanned admission or readmission to the hospital. In each of the SDD and SDA groups, one patient was admitted or readmitted within the 30-day postoperative period. In the SDA group, one patient was readmitted within the 30-to-90-day postoperative period. Other statistics include the following:
- SDD unplanned admission within 30 days: One patient was admitted for dysphagia. The patient was treated with a steroid taper and a soft diet and was discharged home after two days.
- SDA readmission within 30 days: One patient was readmitted for orthostatic hypotension and syncope. The patient was treated with fluid resuscitation, but the orthostatic hypotension persisted. Further cardiac workup (including echocardiography) was normal, and the etiology was deemed to be vasovagal syncope in the context of valsalva.
- SDA readmission within 30 to 90 days: One patient was readmitted for recurrence of symptoms and underwent a revision cervical surgery.
There was no significant difference in unplanned admission or readmission rates for the SDD and SDA groups, either the 30-day admission rate (0.8 percent vs. 0.3 percent) or the overall admission rate (0.8 percent vs. 0.6 percent, p = 0.86).
This study demonstrated that ACDF patients who are discharged on the day of surgery according to well-designed guidelines do not experience higher unplanned admission rates. As outpatient ACDF becomes more common, these protocols can be used to help ensure safety for a growing number of patients.
The criteria for same-day discharge for ACDF surgery includes the following:
- age less than 65 years
- BMI less than 35 kg/m2
- ASA score less than 3
- no history of coagulopathy or bleeding diathesis
- no history of CVA or TIA
- surgery on 1 or 2 spinal levels
- primary (not revision) surgery
- operating room time of less than 180 minutes
- no operative complications
- no immediate postoperative wound complications
- no significant postoperative dysphagia
- hemodynamically stable in the PACU without uncontrolled hypertension
- no need for high-dose analgesics
- no respiratory alarm signs in the PACU, which may include difficult airway per anesthesia, inability to wean supplemental oxygen, witnessed obstructive apnea or hypopnea, escalating pain medication requirements, and pain versus sedation mismatch
Total Inpatient Morphine Milligram Equivalents Can Predict Long-Term Opioid Use After Transforaminal Lumbar Interbody Fusion
The aim of this study was to assess the thresholds for postoperative opioid consumption, which are predictive of continued long-term opioid dependence.
The specific sum total of inpatient opioid consumption as a risk factor for long-term use after transforaminal lumbar interbody fusion (TLIF) has not been previously studied.
Charts of patients who underwent a one, two, or three-level primary TLIF between 2014 and 2017 were reviewed. Total morphine milligram equivalents (MME) consumed were tabulated and separated into three categories based on receiver operating characteristic (ROC) curve analysis of opioid utilization at 6-month follow-up. Multivariate binary regression analysis assessed these MME dosage categories. A further subanalysis grouped patients on the basis of whether they had used opioids preoperatively.
One hundred seventy-two patients met the inclusion criteria and were separated into the following 3 groups:
- less than 250 total inpatient MME (44 percent)
- between 250 and 500 total inpatient MME (26 percent)
- greater than 500 total inpatient MME (27 percent)
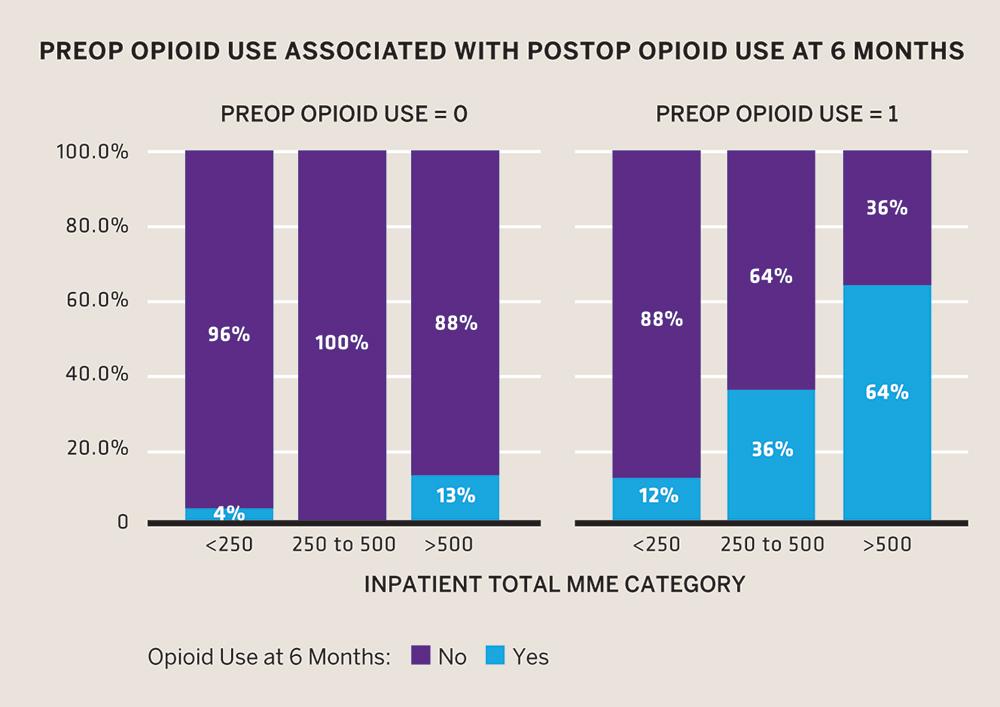
Exceeding the threshold of 500 total MMEs in the immediate postoperative period after a TLIF can predict continued opioid use at 6-month follow-up, particularly among patients with a history of preoperative opioid utilization.
Patients undergoing a TLIF who received less than 250 total MME in the immediate postoperative period had a 3.73 (odds ratio) times smaller probability of requiring opioids at 6-month follow-up (p = 0.027, 95 percent CI 0.084–0.86), while patients who received more than 500 total MME had a 4.84 times greater probability (p = 0.002, 95 percent CI 1.8–13) of requiring opioids at 6-month follow-up.
Exceeding the threshold of 500 total MMEs in the immediate postoperative period after a TLIF is a significant risk factor that predicts continued opioid use at 6-month follow-up, particularly among patients with a history of preoperative opioid utilization.
Osteochondral Lesions of the Talus: Early Failure of Allograft Compared to Autograft in Osteochondral Transplantation
For patients with osteochondral lesions of the talus (OLT), both osteochondral autograft transplantation (OAT) and osteochondral allograft transplantation (OCA) are viable treatment options. However, little research has been done to compare the early failure rates of the two approaches. In this study, surgeons at NYU Langone performed a retrospective analysis to assess early outcomes of OAT and OCA.
All patients in the study were given the option of OAT or OCA after a discussion of the risks and benefits of each procedure. Graft choice decisions were based on patient preference. Data were collected on patient age, patient gender, duration of symptoms, follow-up time, lesion size, lesion location, the presence of cyst in the lesion, previous ankle procedures (including bone marrow stimulation), and concomitant procedures. Clinical outcomes were evaluated using the Foot and Ankle Outcome Score (FAOS) and the Short-Form 12 Health Survey (SF-12) preoperatively and at final follow-up. These evaluations were performed by an author who was blinded to the surgical procedures and radiological analyses. Postoperative MRI was evaluated using the Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) score by a board-certified musculoskeletal radiologist who was also blinded to the surgical procedure and clinical outcome scoring. The rates of cyst occurrence, graft degradation, graft failure, and revision surgeries were evaluated.
The OAT procedure provided significantly stronger clinical and MRI outcomes than the OCA procedure. The rate of chondral wear on MRI was higher with OCA than with OAT. In addition, OCA had a higher incidence of failure than the OAT procedure. These results raise concerns about the biological potential of osteochondral allograft transplantation for the treatment of OLT.
Midterm Outcomes of Bone Marrow Stimulation for Primary Osteochondral Lesions of the Talus
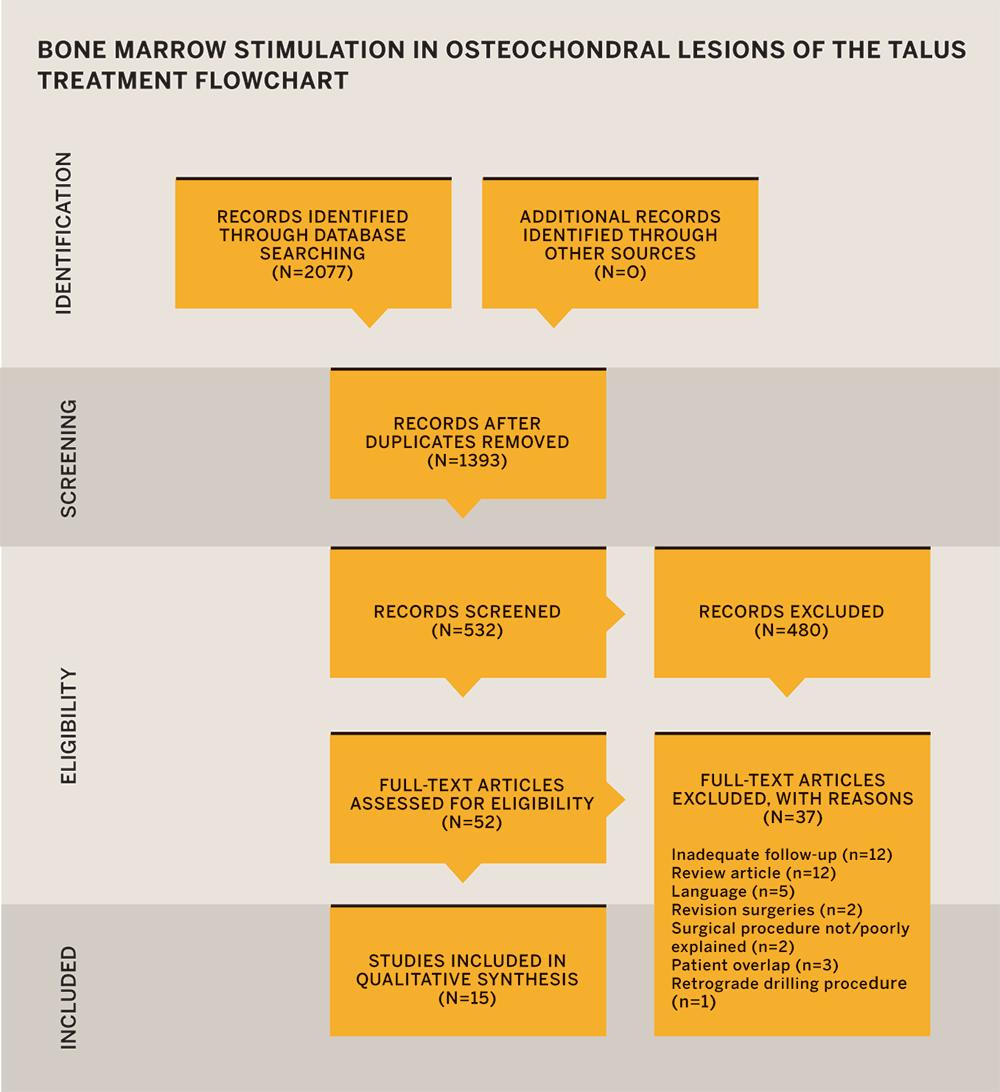
Arthroscopic bone marrow stimulation (BMS) is the most common reparative surgical intervention for the treatment of small osteochondral lesions of the talus (OLT). This procedure has shown favorable short-term clinical outcomes, but the evidence on longer-term success rates is inconclusive. While good mid- to long-term outcomes following BMS have been reported, several recent studies have shown less satisfactory results due to post-procedure deterioration of fibrocartilaginous repair tissue. A lack of evidence on the success rates of BMS at midterm and long-term follow-up still persists.
NYU Langone researchers performed a systematic search of the MEDLINE, Embase, and Cochrane Library databases in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The search identified 15 studies containing 853 patients with a weighted mean follow-up time of 71.9 months. The average patient age was 35.3 years, and the weighted mean lesion size was 110.5 mm. Reported data were variable.
Following BMS in the treatment of primary OLT at midterm follow-up based on the AOFAS score, the midterm complication rates were relatively low, and the data showed a reoperation rate of 6 percent at midterm. Radiological and MRI outcomes may suggest recurrence and reoperation in the long term.
- Nine studies used the AOFAS Ankle-Hindfoot Scale. Among these studies, the weighted mean postoperative AOFAS score was 89.9.
- Six studies showed both preoperative and postoperative AOFAS scores. Among these studies, the weighted mean AOFAS score improvement was 24.5.
- Four studies used the Visual Analog Scale (VAS). In these studies, the weighted mean preoperative and postoperative VAS scores were 7.2 and 2.4, respectively.
- Three studies measured postoperative MRI results at midterm using the Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) system. These studies showed 48 percent complete filling, 74 percent complete integration, 76 percent surface damage, and 78 percent inhomogeneous repair tissue.
- Across all studies, there was a complication rate of 3.2 percent and a reoperation rate of 6 percent following BMS at midterm.
This systematic review found strong clinical outcomes following BMS in the treatment of primary OLT at midterm follow-up based on the AOFAS score. The midterm complication rates were relatively low, and the data showed a reoperation rate of 6 percent at midterm. However, radiological and MRI outcomes did not show similarly positive results, which may suggest recurrence and reoperation in the long term.
The Impact of Socioeconomic Factors on Outcomes Following Anterior Cruciate Ligament Reconstruction
Research has shown that socioeconomic variables can affect patient outcomes for several surgical procedures. The purpose of this study was to assess the impact of socioeconomic factors on one of the most common orthopedic surgeries—anterior cruciate ligament reconstruction (ACLR).
A team of researchers conducted a retrospective query of patients who underwent primary ACLR surgery at NYU Langone from 2011 to 2015 and had a minimum of two years of follow-up. Patient demographics, insurance type, worker’s compensation status, surgical variables, International Knee Documentation Committee (IKDC) score, and failure were recorded from chart reviews. Education level and income were obtained via phone interviews. Inclusion criteria included ACLR with or without meniscus pathology. Exclusion criteria included revision surgery, additional ligament surgery, osteotomy, or refusal to provide socioeconomic data. Statistical analysis across socioeconomic subgroups was performed for patient demographics, surgical variables and outcome using t-tests, ANOVA with pairwise analysis, and linear regression.
A total of 266 patients fulfilled the study criteria. Patients were predominantly male (n = 168) with a mean age of 31.9 years. Medicaid patients had a greater duration between time of initial knee injury and surgery compared to the non-Medicaid group (12.0 [± 16.7] months vs. 6.1 [± 16.5] months, p < 0.001). The mean follow-up time was 3.1 (± 0.7) years after surgery. The mean IKDC score at the time of follow-up was 81.3 (± 15.3). There was no statistically significant difference in IKDC scores between the Medicaid group and non-Medicaid group. When controlling for age, sex, BMI, and the duration between injury and surgery, each income bracket was associated with a significant increase in IKDC score compared to the lowest income bracket.
Socioeconomic variables correlate with significant differences in short-term outcome following primary ACLR. NYU Langone faculty are working closely with public health officials to identify and eliminate the etiologies of outcome disparities related to resource inequality.
Risk Factors for Recurrent Instability or Revision Surgery Following Arthroscopic Bankart Repair
While recurrent instability has been associated with arthroscopic procedures, arthroscopic stabilization remains widely used in the treatment of primary and recurrent glenohumeral instability. One study reported a failure rate of 19 percent following arthroscopic Bankart repair—even with the utilization of modern techniques. As a result, there has been renewed interest in open surgery for glenohumeral instability, particularly for treating patients who are considered high risk of recurrent instability. The study, conducted at NYU Langone, was to identify factors that predispose patients to recurrent instability and revision procedures after arthroscopic Bankart repair.
The team conducted a query of New York state’s Statewide Planning and Research Cooperative System (SPARCS) database to identify patients with anterior glenohumeral instability who underwent isolated arthroscopic Bankart repair from 2003 through 2011 and who were followed for a minimum of three years. In addition to baseline demographic data, the team collected data on the number of ipsilateral closed reductions before initial arthroscopic Bankart repair, evidence of instability of contralateral shoulder, and further surgery to the ipsilateral shoulder.
During the study period, which included 5,719 patients, the number of isolated arthroscopic Bankart repair procedures performed increased by 342.9 percent, from 233 in 2003 to 1,032 in 2011. The mean patient age was 24.9 (± 9.3) years, and 70.2 percent were male. A total of 461 patients (8.1 percent) underwent an additional procedure involving the ipsilateral shoulder for instability at a mean of 31.5 (± 23.9) months after the original procedure. The most common successive surgical procedure was revision arthroscopic Bankart repair, which accounted for 64.8 percent of the subsequent procedure. Significant risk factors for recurrent instability were as follows:
- age < 19 years (odds ratio of 1.86 in comparison to older patients)
- Caucasian ethnicity (hazard ratio of 1.42)
- evidence of bilateral instability (hazard ratios of 2.17)
- history of closed reduction(s) before initial repair (hazard ratio of 2.45)
In addition, revision arthroscopic Bankart repair had a higher rate of continued instability than revision procedures managed with open stabilization (12.4 percent vs. 5.1 percent, p = 0.041).
Previous research about the causes of failure after arthroscopic Bankart repair has been inconclusive. This study determined that younger age, Caucasian race, bilateral glenohumeral instability, and closed reduction(s) before initial repair were independent risk factors for the requirement of a further instability procedure.

