


With a meticulously planned collaborative approach, backed by extensive surgical expertise and preoperative preparation, Dr. Nader Moazami and Dr. Zachary N. Kon provide coordinated care for a patient who needed a multiorgan transplant.
Photo: NYU Langone Staff
A 34-year-old woman in Manhattan sought a second opinion at NYU Langone for deteriorating function attributed to familial interstitial lung disease diagnosed in infancy, mitral valve prolapse (MVP) diagnosed in middle school, and subsequent pulmonary hypertension. She was treated from childhood at the same institution where her older brother had died awaiting a lung transplant seven years earlier. Her brother’s death left her reluctant to pursue a transplant even though her symptoms were worsening.
An Active Lifestyle Despite Functional Decline
The patient’s childhood was marked by episodes of cyanosis and dyspnea, yet she maintained fairly normal activity throughout early adolescence, although she could not participate in sports. She was diagnosed with mitral regurgitation during middle school. Disabling joint pain in high school led to an additional diagnosis of arthritis and suspected connective tissue disease.
Initiating chemotherapy for 6 months at age 18 failed to halt her symptom progression, but a year-long cycle of Remicade® ultimately resulted in remission that lasted through her college years. The patient reported significant improvement and found an engaging field of study, leading to a career with a large international banking organization. However, after more than a decade, she noticed some new shortness of breath and unusual fatigue that prompted an evaluation by her physicians for pneumonia.
Her chronic interstitial lung disease and significant progression of her mitral valve disorder had resulted in heart failure. Treated with three rounds of antibiotics for a presumed respiratory tract infection, her lung function and quality of life continued to deteriorate. In January 2019, she sought a second opinion at NYU Langone.
Pulmonary Hypertension and Progressive Mitral Valve Dysfunction Exacerbate Symptom Progression
Initial evaluation at NYU Langone revealed that the patient’s left ventricular function had significantly deteriorated from longstanding untreated severe mitral regurgitation. Additionally, her right ventricular function was significantly compromised under the strain of pulmonary hypertension secondary to her mitral valve disease and longstanding pulmonary fibrosis. It became clear that a lung transplant would not suffice; she would need a heart transplant as well.
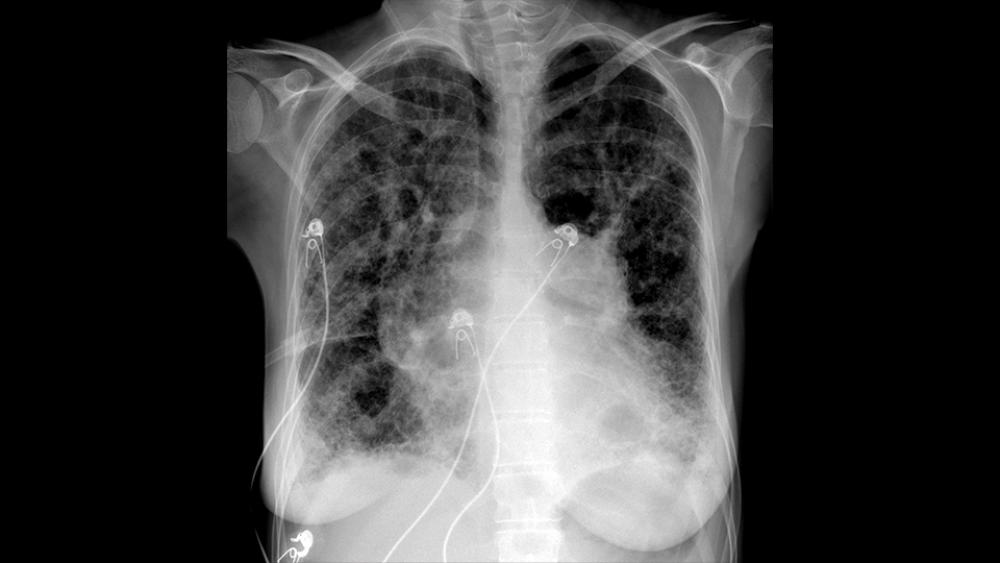
Preoperative X-ray shows an abnormally enlarged heart, with severely enlarged central pulmonary arteries (consistent with pulmonary hypertension), and severe diffuse abnormality in the lungs, which is consistent with underlying chronic interstitial lung disease and pulmonary fibrosis.
Image courtesy of Larry A. Latson Jr., MD, MS
Chest radiography exhibited expected evidence of chronic interstitial lung disease consistent with the patient’s prior CT exam. The images also revealed cardiomegaly, radiographic evidence of pulmonary hypertension, and a large pulmonary artery aneurysm of 3.5 cm. Pulmonary function studies were consistent with severe interstitial lung disease with an obstructive component, with a diffusing capacity of the lungs for carbon monoxide (DLCO) of 14 percent of predicted, and significant reductions in forced vital capacity (FVC) and forced expiratory volume in the first second (FEV1), with a ratio of 53.
During a walk test, the patient’s oxygen saturation on 3 L dropped from 91 percent to 84 percent. Although the patient had accommodated somewhat to lifelong hypoxemia, she was advised to increase her use of supplemental oxygen despite the reluctance she attributed to lack of significant symptomatic relief.
Streamlined Approach Accommodates the Patient’s Personal Priorities
Because the patient continued to work at a demanding pace, the heart–lung transplant team coordinated efforts to accommodate her schedule while she began an extensive evaluation. The potential complications and prognostic data made her reluctant to receive a transplant, but, after exploring her options with Luis F. Angel, MD, medical director of lung transplantation, and Alex Reyentovich, MD, medical director of heart transplantation, she was realistic about the necessity to proceed. The patient noted that the team worked throughout the entire process seamlessly, something she had not experienced despite her long involvement with another healthcare system.
Identifying the pulmonary artery aneurysm and progressive mitral regurgitation with heart failure resulted in the decision to proceed with a heart–lung transplant using cardiopulmonary bypass (CPB). The complexity of the bilateral orthotopic heart–lung transplant after en bloc dissection of the donor heart–lung allograft necessitated a well-coordinated team effort by Zachary N. Kon, MD, surgical director of lung transplantation; Nader Moazami, MD, surgical director of heart transplantation; and Deane E. Smith, MD, associate director of heart transplantation. Careful preoperative planning allowed the team to minimize ischemic time during the transplant.
Function Restored After a Rapid Recovery and Intensive Rehabilitation
After a successful transplant, the patient was weaned without complication from CPB, demonstrating excellent biventricular and pulmonary function before being transferred to the intensive care unit (ICU). Extubated the next day, she was soon ambulatory and working with physical and occupational therapy. After a brief recovery period in the ICU and a short stay at Rusk Rehabilitation, the patient returned home within two weeks, continuing therapy as an outpatient.
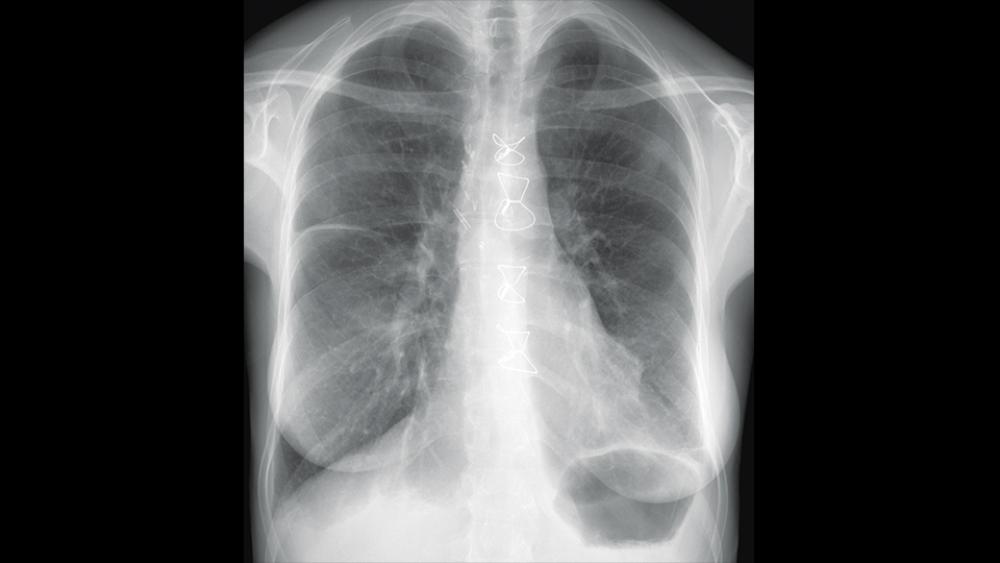
Postoperative X-ray shows a normal transplanted heart size. Aside from some small pleural effusions and a little atelectasis in the lower lungs, the transplanted lungs are normal in appearance. Sternotomy wires and surgical clips appear in the middle of the chest, as is consistent with heart and lung transplants.
Image courtesy of Larry A. Latson Jr., MD, MS
The heart and lung transplant team’s commitment to integrating the patient’s unique healthcare needs with her personal and professional goals enabled her to rapidly recover and achieve restoration of function. She has returned to a challenging work environment and once again has the energy to engage fully with friends and family.
When asked for a summary statement about her experience and her feelings during her recovery, the patient responded unmistakably enthusiastically about how great she felt. She said:
“This outcome was unimaginable to me, but it was clear that the NYU Langone team maximized areas of individual expertise and knowledge across several fields. This expertise increased exponentially from unique shared knowledge developed over time, which enabled the team to envision creative solutions to difficult problems, and to move forward seamlessly and confidently towards a solution, ultimately completing my complex procedure with success.”
Procedure Marks Milestone for Organ Transplantation in New York State
This combined heart–lung transplant was the first performed in New York state in a decade. In 2018, only 32 combined heart–lung transplants were performed in the United States. These complex procedures are reserved for patients who have end-stage disease of both organs, including patients with irreversible right-heart failure secondary to pulmonary hypertension.
The procedure requires intensive coordination between the patient, family, and the NYU Langone Transplant Institute, as well as fully integrating the heart and lung transplant teams. This integrative model—inclusive of highly skilled cardiologists, cardiac surgeons, thoracic surgeons, pulmonologists, social workers, dieticians, pharmacists, nurses, pathologists, and administrative support staff—facilitates NYU Langone’s ability to perform multiorgan transplants.
In 2019, the team has performed five combined heart–lung transplants and anticipates a continued steady volume of cases.
